COVID-19 in Sask: Health officials say it's too early to predict when pandemic will peak
SHA preparing for between 3,000 and 8,000 deaths based on "what-if" scenario modelling

The Saskatchewan Health Authority (SHA) says it is too early to tell when the COVID-19 pandemic will peak in the province,but research from theCanadian Medical Associationprojectsit could happen between early June and late July, depending on the rate ofself-isolation in the province.
On Wednesday, theSHA released itsprojections for the trajectory of the pandemic in adocument titled Health System Readiness for COVID-19.
According to the report, the authority is planning for approximately 3,000 to 8,300 deaths,and approximately 20 to 200 daily intensive care admissions, from COVID-19 at its peak. The SHA has stressed it is planning for worst-case scenarios that are more serious than what the province is currently experiencing.
The document does not include any indication of how long physical distancing measures are expected to continue or when the pandemic is expected to peak in Saskatchewan.
Read the full document here:
(PDF KB)
(Text KB)CBC is not responsible for 3rd party content
Officials in other provinces, such as Alberta, have provided an estimated time framefor when they expect the pandemic to peak locally.
Saskatchewan Health Authority officials said in a news briefing they do not have enough information to make that prediction, because theprogression of the pandemic here is behind that of otherjurisdictions like Alberta.
"We are on a better trajectory than in our 'what-if' scenarios but at the moment we do not have enough information to know for certain," said Dr. Jenny Basran, the health authority's senior medical information officer, in a news briefing Wednesday morning.
Sheadded that worst-case scenario planning is needed because other regions have experienced rapid increases.
Canadian Medical Association releases projections for outbreak peak
Premier Scott Moe said he does not know when the peak of the outbreak will happen in Saskatchewan.
"My estimation would be some time after a number of other provinces in Canada," Moe said at a news conference Wednesday afternoon.
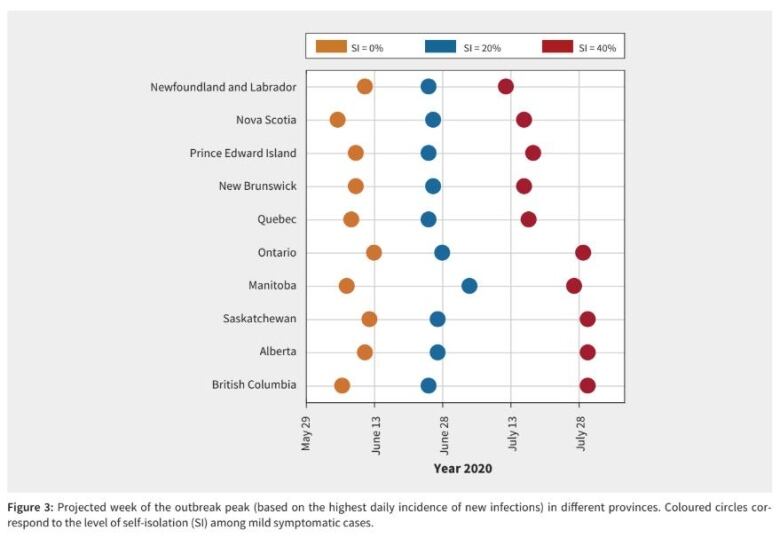
An early report released by the Canadian Medical Association Journal on Wednesday included projections for when the outbreak mght peak in Canadian provinces.
The report, which is titled "Projecting demand for critical care beds during COVID-19 outbreaks in Canada" and is subject to review, predicts the peak would occur between early June and late July in Saskatchewan, depending on on the level of physical distancing in the province.
It predicts the peak in the province would occur in early Juneif there iszero per cent self-isolation, late June with 20 per cent self-isolation, andlate July or early Augustwith 40 per cent self-isolation.
The graph is based on highest daily incidence of new infections.
The report includes a list of data limitations.
"As the outbreak progresses locally, control measures will be adapted and possibly expanded, which may change the trajectory of the outbreaks and would therefore affect our results," it reads.
Saskatchewan chief medical health officer Dr. Saqib Shahab said Wednesday afternoon thathe is aware of modelling released by journals in Canada and the U.S.
"It does show a peak towardMay, June, July and that's many Canadian provinces as well as some U.S. jurisdictions," Shahab said.
"Our modelling group out of the University of Saskatchewan and working with the Saskatchewan Health Authority, has proposed projections that arecontextualized [for] the Saskatchewan environment that really focuses on inputting data that we have already with our 200 or so cases, but also inputting data from other Canadian provinces and other parts of the world."
Dr. Shahab reiterated that physical distancing and other measures will affect the outcome, and that projections and responses will be adjusted depending on the trajectory of the outbreak.
Officials said they would have more information to offer in coming weeks, but the decision on when to release an estimate on the peak is made by the province's chief medical health officer, Dr. Saqib Shahab.
SHA CEO Scott Livingstonesaid physical distancing is making a "large impact" and will flatten the curve if it continues.
"Butit's important for everybody to understand, the more you flatten the curve the longer we stretch this out, and that's intentional," said Livingstone.
"It's so we avoid those peaks that we've seen around the world where health care systems are completely overwhelmed."
The SHA's document stresses that "dynamic modelling is not predictive, rather it provides information to support response and preparedness."It saysit looks at "what-if" scenarios to estimate COVID-19 transmission, the impact of public healthinterventions and impact on acute care demand.
Preparing for the worst
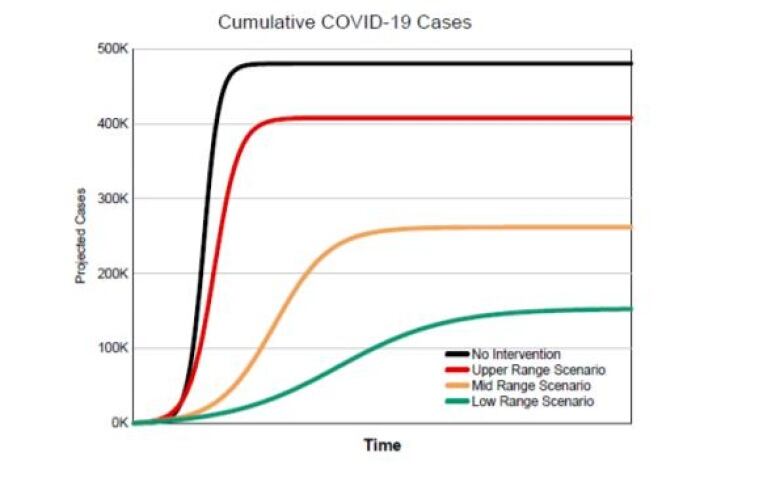
Using three scenarios based on outcomes in other regions, such as Wuhan, China, and parts of Italy, thedocument estimates between 153,000 and 408,000 total cases in Saskatchewan. At best, it estimates 20 ICU admissions per day, at worst it could reach215.
If 153,000 people contract COVID-19 the "lower-range" scenario the documentestimates 3,075 people would die.Under the "mid-range" scenario of 262,000 cases, it estimates 5,260 deaths. And in the "upper-range" scenario of 408,000 cases, it estimates 8,370 deaths. The projections are lower than those released in a draft SHA document leaked to media in March,which projected up to 15,000 deaths as the worst-case scenario.
Dr. Basransaid internationalmodels from regions with different populations have been used because there is no direct comparisonon which Saskatchewan can base itspreparations.
She said models were created with assistance from University of Saskatchewan computer science professor Nathaniel Osgood.
ICU beds to increase from about 90 to 900
"The question that we worked on with Dr. Osgood's lab was really to say,'What if this situation were to happen here? What do we need to plan for and how do we need to be prepared, both from the offensive and the defensive approach?'" she said.
The province currently has 450 ventilators, about half of the 860 it expects it might need. According to the document, there are confirmed orders for 200 more, including 100 expected in the next two to three weeks.
"The ministry are working with vendors and the federal government to close this gap," reads the document.
A graph in the document shows the number of COVID-19 cases per 100,000 people is lower than in most provinces, excluding Manitoba.
The document reveals that more than 1,000 new beds have been opened up to date. SHA's strategy includes plans to increase intensive care beds from 98 to 963 "as needed."
It has plans in place to create dedicated spaces for COVID-19 patients and to create designated COVID-19, non-COVID-19 and mixed hospitals, as required.
Questions remain
NDP Opposition Leader Ryan Meili said the modelling document is an acknowledgement from the SHA that the COVID-19 situation is very seriousand that the authority is willing to talk about itwith the public.
He said he still has unanswered questions about the logistics of the plans.
"How are they going to be moving patients [in rural and remote areas]into larger centres where places are over-capacity and is there going to be anywhere to be doing cohorting?" said Meili.
"If they aren't able to have separate facilities then how will they be cordoning off facilities and making it very safe to have patients who are not COVID positive in the same hospital?"












_(720p).jpg)


 OFFICIAL HD MUSIC VIDEO.jpg)
.jpg)


























































































